A common pelvic organ condition that can worsen if left unattended.
Uterovaginal prolapse happens when the womb drops from its normal position due to a weakened pelvic floor and presses on the vagina, which also prolapses.
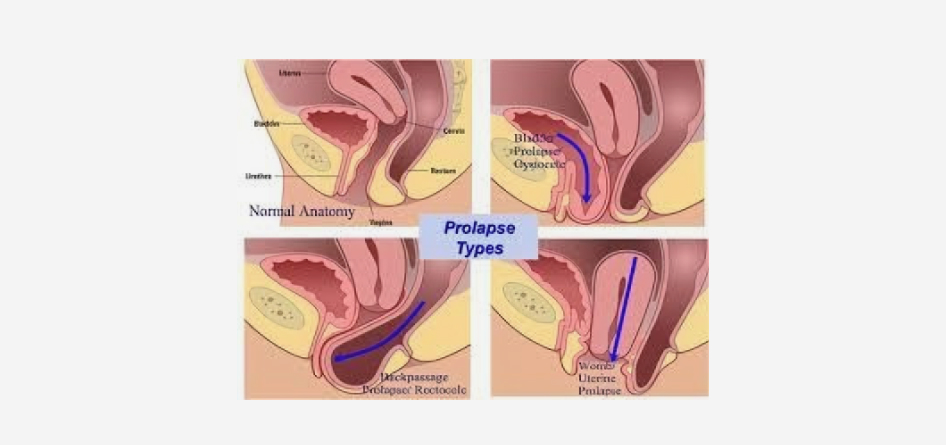
There are five types of uterovaginal prolapse, depending on the pelvic part that presses on the vagina. Uterine prolapse (womb and cervix), apical prolapse (vagina vault drops after removing the womb surgically), anterior wall prolapse (bladder), posterior wall prolapse (rectum), and small bowel prolapse (part of the small intestine).
Factors that increase the risk of prolapse are having a difficult vaginal childbirth (prolonged, large baby), tissue atrophy because of aging, increased abdominal pressure due to chronic obesity or constipation, and connective tissue disorders.
Uterovaginal prolapse is not uncommon in women over 50. At an early stage, it may cause no or only mild symptoms, but if the condition progresses, they will worsen and become discomforting. Those symptoms are:
A feeling of heaviness in the lower tummy or vagina
A bulge or lump in your vagina
Pain or discomfort during intercourse
Constipation
Frequent urination or leaking after a cough or sneeze
If you experience severe symptoms, please see a specialist as soon as possible.
Uterovaginal prolapse is diagnosed and its stage identified through a pelvic examination after taking into account the combination of suspect symptoms, clinical history, and existing risk factors.
The recommended treatment for mild conditions (stage I-II with minimal symptoms), poor surgical candidates, and women wishing to preserve fertility includes pelvic floor muscle training (Kegel exercises) and significant lifestyle changes (losing weight, cutting smoking, treating chronic constipation or cough). Another non-surgical approach is the use of a pessary, a removable device inserted into the vagina to support the prolapsed organ.
When the symptoms severely impact the quality of life or lead to complications, such as ulcers or bleeding, we can intervene either by vaginal or robotic surgery, attaching a surgical mesh to keep the prolapsed organs in place.
For appointments, call my office every Thursday between 9.30 and 15.30.



